What is it?
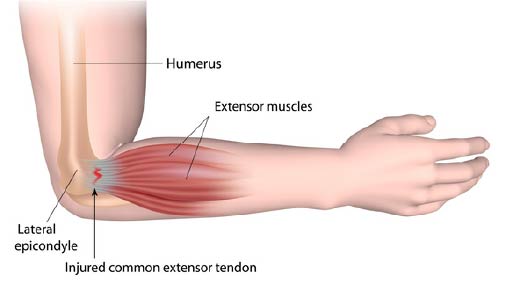
Tennis elbow, otherwise known as lateral epicondylalgia is a tendon injury of the common extensor origin, which connects the forearm extensors to the lateral elbow. The most affected tendon is the Extensor Carpi Radialis Brevis (ECRB). Symptoms are often persistent, with 20% of patients experiencing ongoing disability 3-5 years following onset (Bisset et al., 2015)
What causes it?
Overuse is the main driving factor in tennis elbow, however just like all tendinopathies, other factors can contribute to an increased risk. These include previous hand/arm injury, oral corticosteroid use, reduced forearm strength and poor gripping technique.
How is it diagnosed?
Most cases can be diagnosed clinically with the following findings:
- Reduced grip strength and pain when arm is in extension and pronation. Many patients will have normal grip strength with the elbow bent.
- Painful middle finger extension against resistance.
- Pain on extensor muscle stretching with the wrist in flexion.
Differential diagnoses:
- Elbow OA: will present with restricted elbow range of motion, particularly in older patients with a history of manual work. Patient’s with tennis elbow will rarely have reduced elbow joint range of motion, except in very chronic cases where the ECRB can merge with the lateral and annular ligaments of the elbow. Elbow OA can be excluded with x-ray.
- Elbow chondral injury or loose body: can present with clicking or catching upon elbow flexion/extension in the younger patient with a history of trauma (particularly elbow hyperextension injury). Confirmed by MRI.
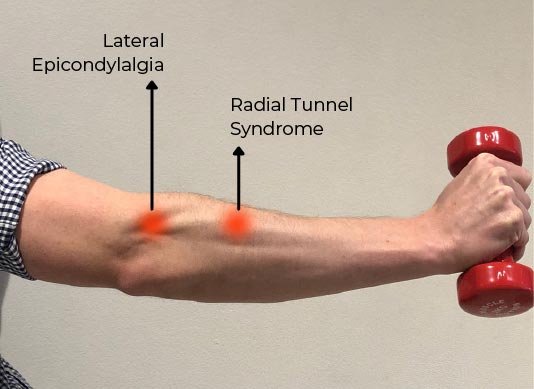
- Radial tunnel syndrome: is the most common differential diagnosis for tennis
elbow. It involves compression of posterior interosseous nerve in the forearm causing pain/burning/tingling in back of forearm and/or hand. Severe cases will have weakness of finger and thumb extensors.
This differs from tennis elbow, where the pain is directly over the lateral epicondyle. Clinically, reduced range of motion on neural tension tests suggests this syndrome. MRI may be used to confirm inflammation in the radial tunnel.
Treatment:
- Forearm strengthening is the mainstay of treatment for tennis elbow, with particular focus on the extensor muscles. (Peterson et al., 2011, Bisset et al., 2006, Coombes et al., 2015).
- Taping and bracing can provide symptomatic relief and allow patients to continue work or activities of daily living until their forearm strength improves.
- Manual therapy specifically lateral glide mobilisations of the elbow have been shown to have both an immediate and sustained effect on reducing pain and improving grip strength.
- Activity modification including rest from provocative activities, as well as educating the patient to lift objects with their palm up rather than palm down

Prognosis (Coombes et al., 2013):
- With forearm strengthening patients are 50% improved after 8 weeks, but to reach 100% often takes 6-12 months in longstanding cases.
- With rest alone patients were 20% improved after 8 weeks and 1/3 of patients will have symptoms beyond 1 year.
Other interventions:
- Corticosteroid injections are no longer recommended. Despite having some effect on short term pain reduction, patients who receive injections have poorer outcome at 12 months compared to no-treatment controls.
- Shockwave therapy may have positive effects on pain in both the short and long term. If combined with strengthening the improvements can be amplified.
- Surgery is the last resort for tennis elbow, with long recovery times and mixed outcomes.









